
Walk-In Acute Care Services
Do you need medical care today, but you can’t get in with your regular Open Door provider?
Open Door is pleased to announce walk-in services for non-life threatening medical issues!
What: Open Door Acute Care Center (ACC) for walk-in appointments for established Open Door patients
Who: for all established Open Door patients. We cannot accept anyone who is not already a patient of Open Door.
Where: 2412 Buhne Street, Eureka, CA 95501 | 707.443.4666 phone
When: 8 am – 5 pm, Monday through Friday (closed for lunch 12:00PM – 1:00 PM)
What: Walk-in health center (no appointment needed) for established patients
Morning appointments accepted before 11:15 AM
Afternoon appointments accepted before 4:15 PM
The ACC serves the following acute issues:
Important Notes:
The Acute Care Center cannot see patients for work related injury or illness, sports physicals, or medication refills of any kind.
We cannot treat life-threatening conditions. If you have any of the following, please call 911 or proceed to the Emergency Department nearest you:
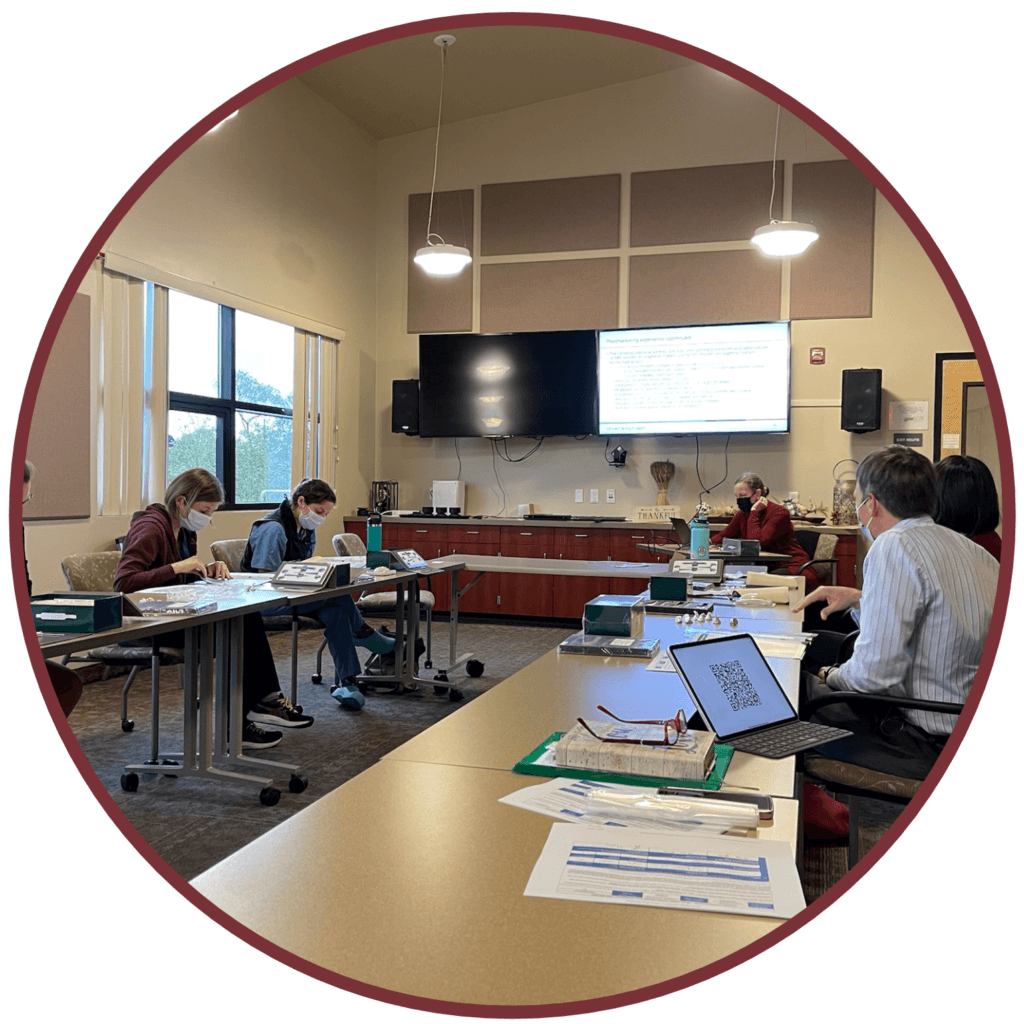
Point of Care Ultrasound Training (POCUS)
The ODCHC APC residency program offers a Point of Care Ultrasound (POCUS) training program as part of our Advanced Practice Clinician (APC) residency curriculum. This program equips healthcare providers with the skills to perform and interpret ultrasounds at the patient’s bedside, resulting in enhanced diagnostic accuracy, timely decision-making, reduced healthcare costs, improved patient experience, expanded access to underserved areas, and opportunities for education and community health promotion. By integrating POCUS into our curriculum, we enhance patient care and access to healthcare while reducing costs benefiting individual patients and the community.
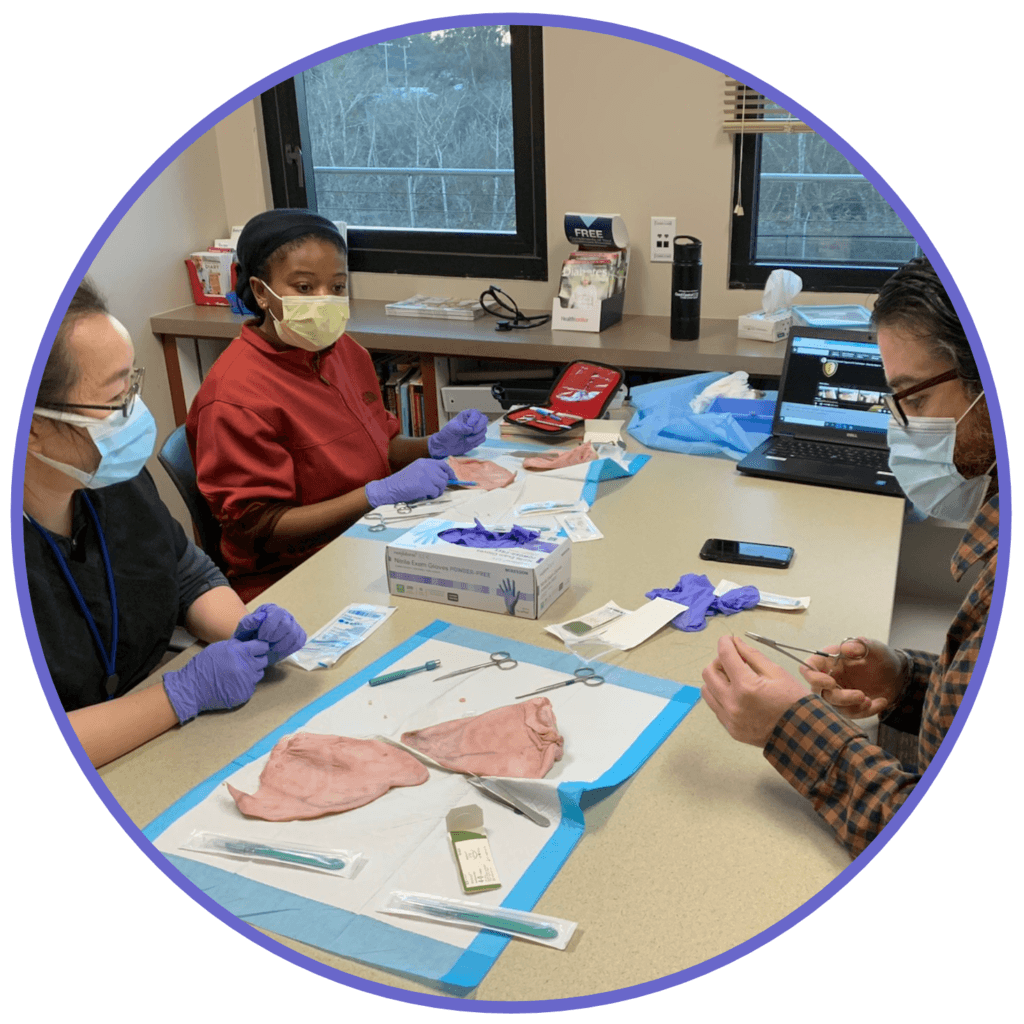
Procedure Clinic
The procedure clinic within our Advanced Practice Clinician (APC) residency curriculum at Open Door Community Health Centers empowers our healthcare providers with the skills to perform essential medical procedures efficiently in the primary care setting, such as biopsies, injections, suturing, etc. This program significantly benefits our patients and community by ensuring enhanced patient care, reduced wait times, cost-effective treatment, and improved access to essential healthcare services. With procedure-trained providers, we prioritize patient well-being, offer prompt and effective procedures, and contribute to our community’s overall health and satisfaction.
Longitudinal Pediatric Clinics
Our Longitudinal Pediatric Clinic training, an integral component of the Advanced Practice Clinician (APC) residency curriculum at Open Door Community Health Centers, is designed to equip our healthcare providers with specialized skills in pediatric care. This program offers numerous benefits to our patients and community by ensuring comprehensive, continuous, and high-quality healthcare for children. Our residents gain expertise in pediatric diagnosis, treatment, and prevention, leading to improved child health outcomes. By focusing on pediatric care, we are committed to enhancing the well-being of our young patients, fostering healthier communities, and providing a vital service to families in need of specialized healthcare for their children.
Humboldt Bay Harbor Cruise (The Madaket)

Humboldt Coastal Beaches and Hiking Trail (moonstone beach, headwater trail, etc)







Redwood Sky Walk at Sequoia Zoo

Applicants must be recent graduates (less than 18 months) from an accredited master’s or DNP program, licensed (CA APRN) and credentialed (FNP-C) or license/credential-eligible as an FNP or PA-C with a stated commitment to practice as a primary care provider in Federally Qualified Health Centers (FQHC) or other safety-net settings upon completion of the residency.
Requirements for newly graduated Nurse Practitioners and Physician Assistants

"The support and continued professional growth offered by the residency program during the often difficult transition from student to provider is priceless. I could not imagine beginning my NP career without it. The organization is welcoming and supportive and the diversity of the patient population provides unique and valuable training opportunities. It has been an outstanding experience I feel lucky to have had the opportunity to be a part of. I wish that all NP’s could have the same supportive start."
Stephanie Randall, FNP

"I love the fact that when I started Residency and decided to stay on board with Open Door, there was and continues to be support available at all times.There is this constant push for excellence and growth; I love that there are constant ways to hone my craft as I am introduced to up to date treatment guidelines.The patient population and their feedback constantly shows me the reward that comes from giving and the need to continue to be better."
Values for Residency:
Marressa Ozokwere, FNP
- Heal and comfort; serve compassionately
- Serve as representatives for Open Doors’ Mission to provide quality care to all people
- Foster growth, excellence and positivity
- Excel at our craft and find ways to continue to improve. View Self-reflection as a strength
- Support and learn from updated research and share with peers; be a lifetime learner
- Treat all equally and responsibly use our power for good

Values of Open Door NP Residency:
- Promotion of a diverse provider workforce representative of the community it serves.
- Dedication to training NP’s to practice at the full extent of their scope.
- Promote provider retention in the field of primary care.
- Training providers to work in a low resource rural practice setting.
- To produce providers that apply their medical knowledge to care for complex medical patients with confidence and compassion.
Testimonial:
“The open door NP residency allowed me to gain confidence taking care of the most complex family medicine patients in a low resource rural practice environment. This program taught me that being a primary care provider is about working as a team at every level to support each other and the patient in achieving their goals of care. The preceptors of this program set the bar for intelligence and compassion, each is dedicated to educating and supporting the next generation of primary care providers”
Angelo Alfano, FNP

Carolina is a Registered Dental Assistant and graduated from College of the Redwoods Dental Assisting program in 2020. Her passion for working with children drew her to the dental van where her engaging communication skills allow her to connect with children of all ages. Carolina enjoys the challenge of turning fearful patients into those who enjoy going to the dentist. With a bubbly personality and attention to detail, she is a great addition to the van team. In her free time, she enjoys dog sitting, spending time with family, and listening to audiobooks (both in English and Spanish).

Luisa is a Registered Dental Assistant and graduated from College of the Redwoods Dental Assisting program in 2019. She has an innate desire to care for others which was cultivated by her strong family ties and caring for her nephew since he was born. Luisa offers a calm and nurturing personality that provides comfort to young children. Her contributions to the van include top organizational skills and always looking for ways to be more efficient, aiding in quick visits. Outside of dentistry, Luisa likes exploring new restaurants and learning how to cook. Luisa is also fluent in Spanish.
Dr. Jennifer Stone is a public health dentist who aims to change the social perceptions of dentistry. She graduated at the top of her class from the Arizona School of Dentistry & Oral Health with a Doctorate of Medicine in Dentistry (DMD) and a Master’s in Public Health (MPH). She has taken countless hours of additional pediatric dental training and education. Her gentle and supportive demeanor allows her to work with fearful and apprehensive young patients. She creates a fun and fear-free zone and prioritizes creating good dental experiences. She utilizes behavioral guidance techniques such as positive self-talk, breathing exercises, distraction techniques, and motivational interviewing. Dr. Stone goes beyond simply treating a tooth by promoting whole-person healthcare which empowers children to care about their overall health and maintain healthy habits for life.
Before coming to Open Door, Dr. Stone created a classroom-based educational curriculum for elementary-aged students in Arizona and Mexico. She has also volunteered hundreds of hours, both domestically and internationally, serving those who need dental care most. Her unwavering commitment to community dentistry has been recognized with several prestigious awards from organizations such as the California Dental Association, the National Health Service Corps, and Rotary International.